Hi! This is Nicole Smith, mom to the “AllergicChild,” or in our case – two allergic children. I’ve received hundreds of emails about my Blog posts about Mast Cells and Eosinophils asking me questions about how to get a diagnosis, which kind of doctor to see, and how to feel better. I decided it is time for me to provide one place for people to find out more about these cells, what happens when things go awry, and how to heal from Mast Cell Activation and Eosinophilic Esophagitis. Or at least, how I’ve found healing through different modalities along with the right medications to calm down my body.
I’m not a medical doctor nor an allergist, but this is what I understand occurs in our body when the body senses an invader, or foreign substance, and the immune system is triggered. An allergy is an overcompensation of the body’s immune system when confronted with the protein of a food, a drug (such as penicillin), a bee sting or an airborne pollen that the body views as an invader. The body releases an overload of histamines in response to the attacker substance, which can create symptoms such as a runny nose all the way to the extreme of anaphylaxis.
The immune system normally protects the body from harmful items such as bacteria or viruses. In the case of allergies, the immune system has a hypersensitivity or an allergic reaction. During an exposure to an allergen, B cells are alerted and turned into plasma cells which produce IgE (immunoglobulin E) antibodies to fight the “invader.” These antibodies travel through the body until they come into contact with the immune cells called mast cells.
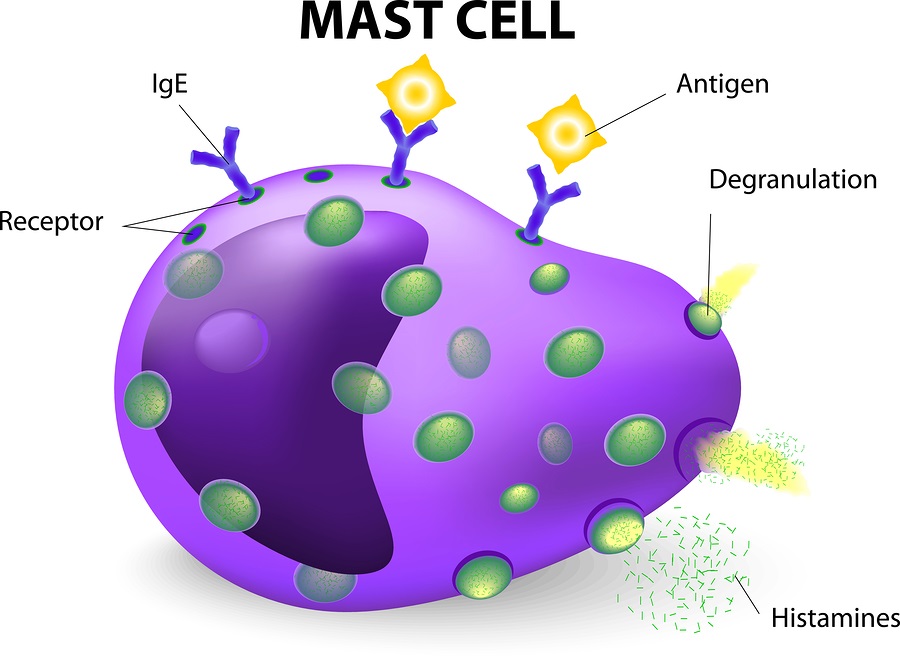
Mast cells are present in the skin, respiratory system and the gut and are important to keep us healthy by fighting off viruses, etc. The antibodies attach themselves to the mast cells via a receptor on the surface and remain attached. That way the next time the immune system meets up with the same invader, the system is primed to react again.
Eosinophils are white blood cells that are one of the immune system components responsible for combating parasites and certain infections. IgE, mast cells, basophils, and eosinophils are essential components of allergic inflammation. Mast cells are tissue resident cells and uniquely required for immediate hypersensitivity. Basophils are largely circulating cells, but home to areas of allergic inflammation during the late phase response. Eosinophils are resident to the GI tract, but also home to allergic inflammatory sites.
Patients with EoE have a high level of white blood cells, or eosinophils, in their esophagus. Research has shown the relationship between high eosinophils and high mast cells. Dr. T. C. Theoharides of Tufts University has found that children with autism have high mast cells, which he postulates causes the severe form of “brain fog” that these patients experience. The brain-blood barrier is compromised and affected by high mast cells. Research has found that patients with untreated Celiac disease have depressed levels of mast cells, as do patients with eczema in different recent research.
Patients with mast cell disorders may or may not have true IgE food allergies; however most of these patients are triggered by high histamine foods. Many are triggered by pollen allergies, and/or certain drugs that increase mast cells. Some, like myself, are so sensitive that food dyes in medications can cause a reaction. It’s interesting that all of these conditions involve mast cells not being “normal.”
Mast Cell Activation Syndrome
Both my grown daughter and I have had a diagnosis of Mast Cell Activation Syndrome (MCAS) for several years. I will share information based upon our experience and our years of meeting with doctors, attending workshops and webinars on the topic, and reading research on MCAS.
You may have heard of systemic mastocytosis or urticaria pigmentosa (also called cutaneous mastocytosis. A gastrointestinal doctor I saw before he retired postulated that there is a spectrum of mast cell disorders that don’t necessarily biopsy in the bone marrow or the skin. One can have a pooling of mast cells in any organ, and my daughter and I have such a pooling in our gut. Patients diagnosed with systemic mastocytosis or urticaria pigmentosa also frequently have stomach aches, since the high mast cell count is not only in their bone marrow or skin, but also frequently found in their stomach.
This same doctor told me that those of us with mast cell issues have a threshold over which we begin to react. This is true with most of the allergic issues. A high pollen day along with a virus can send you or your child’s immune system over the edge to where they break out in hives for no apparent reason. Yet what’s really going on is an onslaught of mast cell activity that has made it appear that you/your child can no longer tolerate certain foods, for example. Or it appears you are having inhalant reactions; or suffering from stomach aches during the Spring and Fall when pollen season is high. Too many mast cells in the body react, and you/your child goes over a threshold, and begin to react to virtually everything.
The immune system threshold may be reached by a virus, a fragrance, pollen in the air, a drug or a high histamine food. If a patient with a mast cell disorder is skin prick tested or blood tested for an allergy, there may not be a true IgE allergy to the “invader.” The mast cells are just “twitchy” and ready to react to anything and everything. These reactions can be in the form of hives, stomach aches or life threatening anaphylaxis.
Patients with mast cell issues may be diagnosed with celiac disease yet find their stomach aches continue even on a gluten-free diet. Or the patient may be diagnosed with Irritable Bowel Syndrome, without any biopsy completed to check for high mast cells in the stomach or intestines. Information about mast cell issues is not in abundance on the Internet.
Most patients with mast cell activation have an abundance of mast cells in the gut. I was told by a doctor that this is because 75% of the immune system is in our gut.
High mast cells in a gut affect the mucosal barrier in the stomach and intestines leading to ‘leaky gut’ syndrome. This allows even more food proteins to pass into the blood stream causing more food allergies and more reactive issues.
From what Dr. Lawrence Afrin stated in a 2019 podcast, Mast Cell Activation Syndrome (MCAS) occurs when mast cells inappropriately produce and release mediators; the increased number of mast cells is fairly modest. The lack of an increased number of mast cells distinguishes MCAS from Systemic Mastocytosis, where mast cell proliferation occurs.
Many patients with MCAS also have excess eosinophils in their gut, and vice versa. Research presented at the 2018 AAAAI conference linked the “atopic march” to EoE. The atopic march describes how patients who have one allergic disease are more likely to develop another or multiple allergic diseases in their lifetime. This progression commonly starts with eczema in infancy and can develop into food allergy, asthma or hay fever in childhood. And the more of these allergic diseases a person has, the more likely that EoE will be a later manifestation of this march. This was important information for me since I had eczema as an infant, had hay fever throughout childhood and into my adult years, and then was diagnosed with food allergies as an adult.
Most of you reading this are probably familiar with asthma – the ‘regular’ asthma that is in the lungs, causing mucous production, coughing and wheezing. Now, imagine if you had asthma in your gut. Asthma of the Gut is the best description I’ve heard yet to explain Eosinophilic Esophagitis (EoE).
In the case of the gut, there is certainly a need for some mast cells to fight off parasite or bacterial infections. The mast cells need to react normally to an invader, and not degranulate at a level causing increased inflammation and chemical release. Eosinophilic disorders create a gut with an abnormally high number of eosinophils in the esophagus, stomach, duodenum, intestines and colon. Inflammation occurs, and the mucosal lining of the gut is damaged creating malabsorption. It is a dangerous cycle to get into.
Research is ongoing to determine the origins of MCAS, however to date no one has yet found a genetic link, or an exact cause. Many patients that I’ve spoke with have detailed a trauma of some sort – a car accident, pregnancy, animal bite, sting, surgery, etc – after which, they began to have the symptoms of MCAS: stomach and intestinal issues, flushing, anaphylaxis, hives, skin rashes, itching, brain fog, rapid heart rate, anxiety and/or swelling.
If you’d like to get even more information about MCAS, I’d suggest the following two books. Dr. Lawrence Afrin has written a book, Never Bet Against Occam: Mast Cell Activation Disease and the Modern Epidemics of Chronic Illness and Medical Complexity that I highly suggest for more detailed information about how mast cells can affect virtually any and all body organs. The book, Mast Cells United: A Holistic Approach to Mast Cell Activation Syndrome by Amber Walker is another great book that enumerates the many body systems affected by MCAS in addition to the numerous other co-existing diagnoses that a patient can have.
To read about MCAS Symptoms and Getting a Diagnosis, click here.