There’s a brand new book out called Allergic: Our Irritated Bodies in a Changing World by Theresa MacPhail. Theresa is a medical anthropologist – who knew there was such a thing ?! – and has done an admirable job covering topics from the medical discovery of allergies, diagnoses, where allergies might source from, treatments, research and more. I’ve just finished reading the book, and I’ve enjoyed reading it, and thought that my AllergicChild readers might benefit from what I found helpful in the book.
I’ve been in the Allergy World all my adult life, and have had years of experience with my own allergies and those of each of my children. Yet, I still learned more about the immune system and how it operates by reading this book. I also learned more about Dupixent and how it came into being. That was a fascinating part of the book to me. I’ve been wondering if it would be a good drug for me to try to combat my Eosinophilic Esophagitis (EoE) diagnosis. This book gave me more details than I’ve been able to find elsewhere. And my conclusion is that the price of the drug is still prohibitive for me!
Ms. MacPhail has interviewed literally dozens of the most esteemed allergists, scientists and researchers for the various topics she covers in this book. If you’ve been part of the Allergy World, you will likely recognize almost all of these individuals. It felt comforting to me that she went to the experts who shared their experience and specific research.
And beyond just the experts, she also interviews parents and advocates who have created groups and non-profits that help individuals in the Allergy World. I liked reading about these individuals, especially since I know them and have met them at food allergy conferences through the years. I respect them tremendously, and reading about them in the book only made me have even more appreciation for them and everything they have done for our community.
If you’re looking to learn more about food allergies, pollen allergies, your immune system and treatments that are on the horizon, I’d definitely suggest you read this book!
(PS – I’m not receiving any remuneration to provide you this review, nor do I know the author. But I would love to have more conversations with her if I ever did get to speak with her!)
This is a blog post that I’ve been intending to write for years. I wanted to share what we’ve experienced about helping our son, Morgan, learn how to manage visiting his allergist while he still lived at home. He could then make good choices about getting an allergist once he was out on his own, and Mom wasn’t around to give directions!
We’ve been blessed that Morgan was able to have the same allergist for 21 years, until he graduated from college. She watched him grow up and to learn to take responsibility for his health. However, it wasn’t until he was 19 years old, as a freshman in college, that he went to the allergist unaccompanied by Mom. Boy did it take work to get to that point!
Morgan visited with our allergist at least every 6 months throughout his life, beginning with his first appointment at 15 months old. He learned the routine of an office visit – fill out the paperwork listing all his medications, have a height and weight check, take a lung function test or two, and visit with the allergist to tell her how he’s feeling.
If Morgan had experienced any type of issue – a cold, virus or a pollen reaction – I wanted him to learn how to use his words to explain what happened. This was good practice for him to be able to explain to any adult what he was experiencing in his body and what he needed to feel better.
It took many years for Morgan to learn how to properly list all his medications that he took for pollen allergies and asthma, and to not forget any of them. He had to know the exact medication name, the milligrams, how often he took the medicine and whether he needed refills. I began having him complete this form when he was in grade school so that he could learn the details of his health needs. He would need to check with me about the answers, but he did all the writing.
Many times he would have school forms or camp forms that needed to be completed. He would complete parts of those forms, and I would fill in the rest until he was able to complete the forms by himself once he applied for accommodations in college.
It is vital that our children know all about their health condition(s), and are prepared to go to the doctor by themselves. Taking the initiative and the time when they are young to allow them to learn about the paperwork will help them later in life when they leave home.
It was at Morgan’s first allergist appointment that he had his first skin prick test. Holding down a wiggly, itchy toddler for 15 minutes was no easy feat!
From that test on, I kept an Excel spreadsheet where I input results from every skin prick, RAST and Immunocap blood test through the years. Every 3-4 years, we had repeat tests run. Because of the number of allergies that Morgan has, it has been helpful for him to refer back to this spreadsheet to see if he’s got an allergy to mold, or to some food that he wants to try. Then he can discuss the allergy test result with the doctor to see if a food challenge is warranted.
Once Morgan graduated from college, and moved to a suburb of Denver, Colorado, he needed to get a new allergist. He searched around and found a physician who knew our allergist. This doctor had been an allergist for over 30 years, and that made Morgan feel more comfortable. Morgan moved again two years later, and once again wanted to find an allergist near his home. This time, it wasn’t as easy to find a good fit. The first doctor he saw said that carrying just one autoinjector – Auvi-Q – was enough. That was enough for Morgan to decide this wasn’t the doctor for him. He knew he needed to always carry two Auvi-Q’s, and the fact that this doctor didn’t state that was concerning enough to leave the practice.
He decided to search for another doctor, and has now found a younger woman that he likes very much. She has redone all of his food allergy testing, and found that he is able to do an oral challenge for almonds. So far, he hasn’t found a desire for this. He continues to have food allergies to peanuts, tree nuts, sesame, fish and shellfish, and continues to see an allergist once a year and ALWAYS carries two Auvi-Qs with him everywhere.
I have full confidence that he knows how to manage his health, and he is fully capable of communicating with an allergist about all of his medical needs. And that was always the goal!
There will be 3 epinephrine autoinjectors on the market effective February 14, 2017: the EpiPen, Adrenaclick and the Auvi-Q. All three devices are available in a Junior strength for children, and an adult strength.
Listed below are the pros and cons of each of these devices based upon my experience and upon the information available on their websites:
The EpiPen has been around since 1977, and owned by Mylan since 2007. There has only been one recall that I’m aware of, which was in 1998 when Meridian Medical Technologies manufactured the device. Almost 1 million devices were recalled since they weren’t providing effective doses of the medication.
The EpiPen training video states that the device needs to be held for 3 seconds after administration.
Pros:
The EpiPen currently has the largest share of the market, which means that more people have been trained on this device than any other.
A trainer comes with every prescription.
The used EpiPen has the needle protected with the orange cap.
Cons:
The price! Currently the brand name 2-Pak is around $600+ without a coupon. The generic EpiPen will cost you $300, and no coupon is available.
With a generic EpiPen available, and the Adrenaclick (generic epinephrine), your insurance company may not cover the brand name drug.
The size. Carrying a 2-Pak is bulky, and many young men really balk at this.
The short lifespan. Generally the EpiPen expires within 12-14 months, and you’ll likely have to ask the pharmacist for the furthest out expiration date to get this.
The Adrenaclick has been on the market since mid-2013. The training video states that it needs to be held for 10 seconds after administration.
Pros:
The cost at CVS pharmacies. With a $100 coupon, the cash price is $9.99.
The lifespan. Adrenaclick’s have an expiration date at least 24 months out.
Less bulky than the EpiPen.
Cons:
No trainer comes with the package. You will need to contact the company and request to have a trainer sent to you. You can do so here.
Fewer people have been trained on the Adrenaclick in school systems and elsewhere. This may change as more people purchase the device and bring it to school, etc.
The cost at approximately $400 with high deductible policies if you don’t purchase the device at CVS.
The needle is exposed after use.
You need to pull both tabs off of both ends of the device before administering it. This can make for confusion as to which end to use for injection, even though it has a red tip. Seconds count in an emergency, and a layperson may have more difficulty with this.
The Auvi-Q was originally manufactured by Sanofi, and was introduced in January of 2013. A recall of all devices occurred in October of 2015 when two dozen of the devices were suspected to have not administered the correct amount of medication. Sanofi no longer manufactures Auvi-Q. Instead Eric and Evan Edwards, the inventors of the Auvi-Q, brought the manufacturing back to their company, Kaleo Pharmaceuticals. Both Eric and Evan, and their children, have life threatening food allergies.
The Auvi-Q training video states that the device needs to be held for 5 seconds after use.
Pros:
The device can talk anyone through the administration of epinephrine.
A trainer comes with a prescription.
Size. It’s about the size of a thick credit card, which makes it easy to carry in a front pocket for men.
Cost. Kaleo is promising $0 out of pocket cost, even for those with high deductible insurance!!
The needle is not exposed after use.
The makers of Auvi-Q have food allergies themselves, as do their children. In other words, they are one of us – the food allergy community AND they have a social conscience when it comes to pricing autoinjectors.
Cons:
The previous recall may be on some people’s minds; however, with the manufacturing moved in-house, I believe this issue has been resolved.
The lifespan of at least 12 months. But if you’re paying $0, I don’t believe that’s as big of an issue!
I was the woman at the end of the video clip who isn’t so thrilled about the Adrenaclick being offered for $109.99, and I’d like to tell you why!
First off, there’s a confusion that the Adrenaclick is the generic EpiPen. This is not true. In fact, a local CVS pharmacy that I called tried to tell me that the Adrenaclick is the generic EpiPen!
(Side note: Mylan is offering the brand name EpiPen as a generic at a $300 price tag for a two-pak. The brand name’s price tag currently runs upward of $600, however there are coupons that can bring the price down by up to $300. Cigna also announced on 1/12/17 that they will no longer be honoring prescriptions for the brand name EpiPen, only the generic.)
If you want your allergist to prescribe an Adrenaclick, you will need to have a prescription specifically written for the medication. And if your allergist is like ours, they may not prescribe it. (More on that later).
Next, to obtain the $9.99 price that’s quoted in the video for an Adrenaclick, you may need to pay out of pocket the $109.99 at CVS, submit a rebate form to the company, and wait for the $100 refund. To me, that’s not the same as a $9.99 price at the pharmacy. And remember you have to purchase the device at CVS in order to get this price.
As I said in the clip, I’ve been trained on the Adrenaclick. It isn’t near as easy as the EpiPen to use, nor is it as easy to train others, (especially since the package DOES NOT come with a trainer). It was for this reason that our allergist was not willing to prescribe Adrenaclick for our son prior to his study abroad in the fall of 2016. With him being in different countries where different languages are spoken, and eating different foods, she didn’t want to exacerbate the issue with him having a new autoinjector that he hadn’t ever used before nor had never trained anyone else how to use.
Many K-12 schools and school nurses are not trained on this device yet. If you plan on purchasing this autoinjector, make sure that everyone who could potentially need to administer it has ample training and feels comfortable using it. What may seem obvious to you or me, as an allergy parent, isn’t so obvious to a school administrator or teacher as far as the difference in this device and the EpiPen.
The Adrenaclick training video states that the device should be held for 10 seconds, instead of the current 3 seconds for an EpiPen. And, if you use the Adrenaclick, the needle remains protruding. I always disliked this about the EpiPen prior to its most recent redesign. I very much like that now the used EpiPen has the needle protected to ensure that no injury occurs after injection.
I am excited for competition in the marketplace, and I’d love nothing more than to have an epinephrine autoinjector cost just next to nothing!
I’m really excited about the reintroduction of the Auvi-Q, which should occur within the next few months. What’s really great about it is that it talks the user through the steps to administering it!
The Adrenaclick is just too similar to the EpiPen to cause enough confusion for the administration of the device to be compromised. It’s not a good alternative for our family.
Hi everyone! It’s Morgan. I’m currently researching small business growth in Denmark at the moment, but I decided to take a quick reprieve from my research and look into EpiPen® pricing here in this country.
Copenhagen!
The recent outrage over Mylan’s price increases certainly has made international news. Heather Bresch is now viewed as a challenger to Martin Shkreli as worst CEO of a pharmaceutical company, ever. Good.
Seeing all the news and congressional inquiries started to make me think: why does the US have this problem? Is it only a US issue? Why can Mylan get away with this blatant price gouging?
Doing a full cross-country comparison among developed countries in North America and Europe would take a few weeks, so I decided to examine how Denmark does it.
Background
Denmark has a publicly funded health care system with mixed governance structures: the national government sets health care goals, policies, and tax structures while regional and municipal governments oversee the delivery of health care and process payments and reimbursements.
All Danish citizens qualify to be a part of the health care system and self-identify into two groups:
Group 1. 97% Danes select to be in Group 1. It’s entirely free to visit a general practitioner (GP), but you need to get a recommendation to visit a specialist. If you visit a specialist upon recommendation of your GP, it’s entirely free.
Group 2. 3% Danes select to be in Group 2. You can visit GPs or specialists at your pleasure and don’t need recommendations. All GP visits are free, but there’s only partial coverage of costs for specialists.
Denmark offers on-the-spot reimbursements for pharmaceutical costs (more on that later) and it doesn’t matter if you’re in Group 1 or 2.
Pharmaceutical Delivery
Let’s say I’m the CEO of a pharmaceutical company. Let’s call this company Molfyne and say it mainly produces anti-depressants. Let’s also assume that I’m licensed by the Danish government to produce and sell pharmaceuticals in Denmark.
Molfyne would need to apply to the Danish Medicines Agency, a national agency, to have its drug recognized and sold in Denmark. I would need to file an application with the Danish Medicines Agency (DMA) and tell them my selling price of my drug to Danish pharmacies. I also submit documentation regarding the effectiveness, side-effects, and value-added of the drug (among other information) to DMA and wait for their response.
DMA determines whether the drug will be reimbursed or not based on those factors. It’s not entirely clear from my research whether DMA “negotiates” with my company over my price offered, but I suspect there might be a little negotiating.
Then, if approved, my anti-depressants are bought either by Denmark’s hospital drug procurement company (called Amgros) or by private wholesalers who sell to local pharmacies. If a patient is prescribed my drug in a hospital, there’s no co-pay or any payment since any and all pharmaceuticals are provided by the hospital and payed for by taxpayers.
If a patient is prescribed my drug by their GP or specialist and needs to buy it from a local pharmacy, they are reimbursed on-the-spot by the Danish government on a tiered system. This means that if a drug cost $50 and they qualified for a “$10 reimbursement,” they would only pay the pharmacy $40. This tiered reimbursement system is determined by how much you’ve spent on pharmaceuticals this calendar year. These tiers are 2015 numbers and are adjusted annually.
(DKK refers to the Danish Krone, their currency; $ is US Dollars)
You pay out of pocket up to DKK 925 ($138)
You get a 50% reimbursement for DKK 925 to DKK 1515 ($138 — $227)
You get a 75% reimbursement for DKK 1515 to DKK 3280 ($227 — $491)
You get an 85% reimbursement for expenses higher than DKK 3280 ($491)
You get a 100% reimbursement for expenses higher than DKK 3830 ($574)
To translate this, if I need to get $200 worth of drugs in February, I pay $138 out of pocket, and get 50% off the remaining $62. But if I need to buy $200 of drugs in June, I get the 50% reimbursement on the leftover of the second tier ($27 worth), and get a 75% reimbursement on the remaining cost. It means the more drugs you need to purchase, the less expensive it gets for you.
There’s only one catch: reimbursements are calculated based on the least expensive generic product. Pharmacies are required to issue the least expensive generic product, unless a doctor says otherwise (this is unusual). So, if your doctors says “not the generic one” you may have to pay a bit more, but it is still heavily reimbursed.
EpiPens in Denmark
Denmark makes it really easy to find out how much drugs cost across the board: they even have a website (http://www.medicinpriser.dk/) you can explore. It is in Danish, but you can select “English” in the upper right to view it in English.
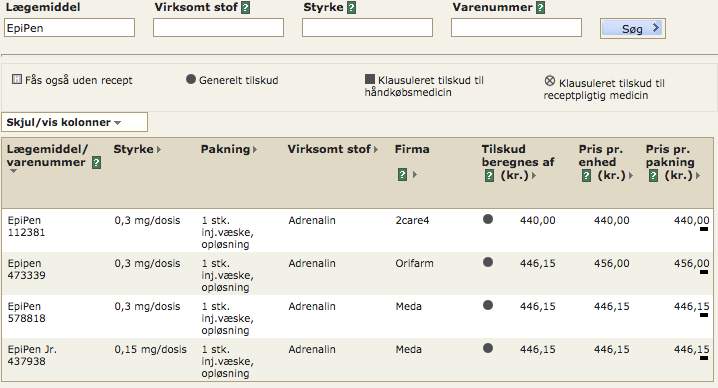
If you search “EpiPen” you get this screen:
Notice that there are three items for 0.3 mg doses (the Stryrke column) from three pharmaceutical companies: 2care4, Orifarm, and Meda (the Firma column). Look at the consumer price (far right column)! 440 DKK is the equivalent of about $66. This means that you would pay $66 for an EpiPen® (a single one, not a two pack). The Meda EpiPen® costs 446.15 DKK, which is about $67. Really not much difference between the companies.
I was blown away seeing this. $66 for one EpiPen is cheap, even though it is an increase from previous years. Furthermore, if I have other drug costs from the year and need to get an EpiPen, this could cost me $33 (50% reimbursement), or ~$16 ($75% reimbursement). That’s quite inexpensive.
Lastly, drug companies are only allowed to adjust prices every other Monday, and they must be publicly recorded with the Danish government. There is also a law-binding agreement between an association of pharmaceutical companies (called Lif) and the Danish Ministry of Health to only raise drug prices ~1.5% every 4 years. Only some companies, like Sanofi and Pfizer, are a part of this association.
What’s the Trade-Off?
Obviously, this lower price for an EpiPen® is not happenstance. But, before we get to taxes, I’d like to note two important changes in the Danish system:
Drugs available to hospitals are negotiated by one sole entity. There is a “monopsony,” a literal single buyer in that market (Amgros). Amgros is the only entity that provides Danish hospitals drugs and therefore drug companies have to negotiate with Amgros to sell their drugs. This means an emergency responder or a hospital does not need to worry about using an EpiPen® since the price is reasonable.
Drug reimbursements are approved by a national health authority, the Danish Medicines Agency. As I clarified earlier, I can’t find too much about the DMA negotiating with drug companies, but I bet they wouldn’t approve reimbursements for drugs that are exorbitantly expensive, which means Danes wouldn’t have access to them by any practical means.
On to taxes.
You pay 8% on all gross income — regular income, wages, pension benefits, and so forth. There are deductions for interest dividends up to about $7,000 a year.
Then, you pay the following national income taxes (2014 rates):
5.83% for incomes between 42,900 DKK to 421,000 DKK ($6,420 to $63,100)
15% for incomes above 421,000 DKK (above $63,100)
You also pay between 23% and 28% to your municipality (averaging about 24% across Denmark). They’re merging their national healthcare contribution tax (3% for 2016) into their national income taxes over the next few years, but you pay that too. In total, you could pay upwards of about 57% of your income to governments of various levels every year. That’s a lot of taxes.
Oh and there’s a 25% value-added tax (kind of like a sales tax) on all goods.
Benefits
The Danish government provides a lot more than just universal healthcare in exchange for those taxes. There’s extensive unemployment insurance, social security, education (including higher education), job training, and vocation schools. Plus you get the “normal” benefits like paved roads and national security. This kind of system is referred to as the “Scandinavian welfare model.”
Lessons for the United States
Health care is a complicated system. There are pharmacies, health insurance companies, pharmaceutical companies, medical device manufacturers, hospitals, emergency providers, private practices, and so much more. Denmark decided to basically keep most of that private (only doctors at hospitals are “public employees”; most health care providers are private employees) but fund it all publicly. They figured out ways to keep regulatory compliance low and efficient.
It’s also important to note there are a lot of differences between the United States and Denmark. Geographic size, population, and regional inequalities all play a role. If you live in a rural region of Denmark, you’re going to get the same kind of schooling or access to health care as kids in Copenhagen — that’s not necessarily true of Mississippi versus Minnesota. Denmark is only 5 million people large; that’s barely the size of Colorado. And, of course, it’s a tiny maritime nation on the north end of Germany versus half of the North American continent.
Nonetheless, I think there a few key takeaways:
The US needs to get serious about price negotiations. The Economist recently ran an article on EpiPen® pricing and the failures of the US system (note: there might be a paywall). It’s illegal for Medicare, our nation’s largest health insurance entity, to negotiate with drug companies on pricing. Only private health insurance companies can do that and they’re heavily constrained in their negotiating — only in 6 broad categories. The idea behind this choice was that competition would result in lower prices, but it obviously hasn’t worked. From the article: “As a result America spends 44% more on drugs per person than Canada, the next-highest.” That isn’t working. A publicly funded entity like Amgros could help lessen the price of drugs across the board, but it’d be very politically unpopular.
The US needs to get serious about pharmaceutical influence in politics. Denmark spends about 9.8% of its GDP each year on healthcare (12.4% of that total expenditure is on pharmaceuticals) and pharmaceutical companies comprise about 13.5% of its exports. Pharma is big in Denmark. To compare, all machinery exported by US companies comprised 13.7% of our exports. The Danish government has every reason to bolster their pharmaceutical industry and loosen regulations, but they don’t. On the flip side, as the Economist article pointed out, “[Mylan’s] chief executive, Heather Bresch, heads the generic-drugs lobby and is the daughter of an American senator.” There’s some questionable influences in American politics over our regulation of and choices regarding the pharmaceutical industry.
Lastly, the US needs to get serious about insurance reform. Drug companies are notorious about offering coupons and deals for many of their more expensive drugs, especially if your insurance doesn’t cover their drug. They do this so they “look good” and can avoid regulation by Washington. But, they don’t do this for insurance companies. Insurance companies have to pay for the expensive drugs without the deals some consumers gets. In the long-run, that raises insurance prices for everyone. The Affordable Care Act (y’know, Obamacare) only did so much to combat that and, in some cases, ran counter to that goal by causing insurance price increases.
We need some serious healthcare reform. Most of it is going to be opposed because (from the Economist, again) “the only thing that Americans detest more than an expensive drug is a bureaucrat who says they can’t have it.” But, there are obvious lessons from countries around the world who have effectively dealt with price gouging by pharmaceutical companies like Mylan.
It has been a firestorm over the last week with consumers, doctors, and the media calling out Mylan for its price gouging of the life saving medication, EpiPen. While Mylan CEO, Heather Bresch, argued that the problem is with the health care system instead of with Mylan in particular, Mylan did come to the PR table to provide further discounts to consumers.
This is too little and too late, especially for the thousands of consumers who have already scrimped and saved to purchase EpiPen 2-Paks for their children to take to school this year. Nothing monetarily was provided for any family who has already made purchases.
Additionally, this appears to be a public relations tool to not only stabilize their stock price (which has dropped almost 11% over the last three days), but also to quell all the media attention.
What should Mylan REALLY do? Here’s what I’d suggest:
Give Heather Bresch her walking papers. She has been a controversial figure with her MBA credentials having been called into question, and the EpiPen price increases were destined to be an issue if anyone had had the foresight to see the writing on the wall. Let her take the fall for this and wipe the slate clean. She has stated that EpiPen is “her baby,” so she is responsible for the price gouging.
Cut the EpiPen 2-Pak price to $300, the price it was in 2013-14. With their new $0 copay card value of $300, this would allow consumers to pay nothing. It would also be decreasing the cost of the product for insurance companies portion of the prescription – which we consumers are still paying in the form of higher premiums.
Make Anaphylaxis 101 a non-profit. It’s going to be difficult for Mylan to find a spokesperson now that both Sarah Jessica Parker has stepped down and Kelly Rudnicki, a Food Allergy Mama, who is a beloved figure in the food allergy world. Making the website Anaphylaxis101.org would allow for some good to be coming out of Mylan toward the food allergy community. And put a few members of the food allergy community on that non-profit board of directors!
To further that thought, Mylan needs to get a PR makeover. The best way to do that is GIVE, GIVE, GIVE to the allergy community and to apologize for what they’ve done with raising the price of EpiPens beyond what American consumers can afford. Americans love a redemption story, and it’s time for the old Mylan philosophy of greed, corporate tax evasion and executive compensation packages to be burned to the ground. What can rise is a new company, with the philosophy of collaboration and innovation.
Lastly, Mylan needs to take the HUGE amounts of profits that they made from EpiPen sales and put the money into research of an auto-injector product that meets the needs and desires of consumers: small, lightweight and a stable shelf life of 2 years or more.
Mylan could be a hero to the Food Allergy World if they’re willing to make amends and give up their current corporate philosophy. Become the company that our children would want to work for! If not….then I cannot wait for the competition that’s forthcoming in the epinephrine auto-injector market!