When my son, Morgan, was a little boy he continued to add more and more food allergies. He started with a peanut allergy reaction – breaking out in hives from touching a peanut butter sandwich at the age of 9 months. Thankfully, he didn’t eat it!
He added an egg allergy after a reaction to the MMR vaccine, and subsequent testing at 18 months old confirmed egg and also confirmed a severe peanut allergy. Our allergist suggested that he not eat tree nuts because of the likelihood of cross contact in the manufacturing process with peanuts.
Then, at the age of 3, he had full body hives and we went back for more testing to determine what food was causing the issue. To our dismay, he added another allergy – shellfish, but he hadn’t eaten shellfish the day of the hives, so we began to suspect sesame as the cause of the hives, but didn’t get that confirmed until a later allergy testing. We had further testing completed a few more times as he got older in the hopes that he would have outgrown a few of these allergies. While he did appear to outgrow egg allergy, it wasn’t until he was in high school that he was willing to go through a food challenge for eggs, which he passed. That was the only food allergy he had outgrown during his childhood.
He wasn’t supposed to be allergic to fish, as per one of the allergy testing results, yet had full blown anaphylaxis to one bite of trout on a camping trip a few years after this testing. That was a shock to say the least! So we added that food to his ever-growing list of food allergies.
He was managing peanut, tree nuts, shellfish, fish and sesame allergies from middle school through college and out into the work world. We basically had given up on him ever outgrowing any of these food allergies.
It has been 2 years since that last food challenge (he’s 30 years old now), and Morgan recently got brave enough to test for hazelnut, which had come back almost negative in two previous allergy testing results. A food challenge can be very anxiety producing, and we’ve found that Morgan has to REALLY want to eat the food to make the process worthwhile. And he really wanted to be able to add another food back into his diet. Also he wanted to be able to eat Nutella!
He went through the allergy testing over several hours at his allergist’s office slowly adding more and more hazelnuts. He did experience anxiety during the testing, but was able to continue to push on through because everything went well. At the end of the day, he passed!
He’s now eating hazelnuts as a part of his diet with no issues! Hooray!
Disclaimer: This post is not medical advice. This article is written from Morgan’s perspective of managing his food allergies to peanuts, tree nuts, sesame, fish and shellfish.
I returned from a trip to Seattle in early September, having educated a bartend at a fairly high-end cocktail bar on how many gins can contain tree nuts, and realized that it might be worthwhile to write a post on navigating alcohol with food allergies. If some bartends don’t even know… I can only imagine where everyone else is!
This is an incredibly expansive topic. It’s made much more complicated by the growth of the “craft” industry (craft beer, craft cocktails, craft cider, etc.) that yields infinite variations in products. I’m going to address a few background items first and then share some notes on specific types of alcohol.
Background Notes
Allergy Labeling
At the end of Prohibition in the U.S., the responsibility for labeling alcohol did not fall to the FDA but a different federal agency, the Alcohol and Tobacco Tax and Trade Bureau (TTB). So as a quirk of history, when the FDA started to regulate nutrition labels in the 1990s on all packaged foods, alcohol was not affected.
This creates an obvious problem – you don’t always know what is inside the bottle or can you’ve purchased. That means you could buy a bottle of Southern Comfort and have no idea it contains tree nuts as a flavoring product. Or, order a cocktail that uses Frangelico (a liqueur) and the bartend couldn’t check the bottle to see it contains hazelnuts.
This makes drinking alcohol a minefield for someone who has one or more allergens. At a different high-end bar we went to, my boyfriend ordered a drink that contained a specialty Vietnamese liqueur. It turns out it contained cashew, but it was only through sheer luck that the producer voluntarily mentioned that ingredient on the label. (For the record, I don’t have drinks with mystery liqueurs so I wouldn’t have been drinking it anyway)
On the other hand, the TTB is notoriously strict about what a producer can put on their label. This is because before (and after) Prohibition, many liquor producers were adding poisonous substances like gunpowder and trying to pass it off as a legit product. In order to restore confidence in products being sold, we forced producers to only use certain terms that indicated a certain quality of production.
Southern Comfort is labeled as “spirit whiskey with natural flavors and caramel color.” Those “natural flavors” include tree nuts derivatives.
Whereas Four Roses, a popular bourbon, is labeled as “kentucky straight bourbon whiskey.” By law, Kentucky straight bourbon cannot contain any added colors or flavors – it must be 40% ABV or higher, aged in new oak barrels for two years, and must be made from at least 51% corn. In this case, it could be a handy rule to avoid anything that says “natural flavors” on the label.
Not all categories are useful. A “London Dry Gin” is a type of gin made with a low amount of sugar (hence, dry) but can encompass gins that are made with almonds (Bombay Sapphire) and those that aren’t (Tanqueray).
Craft Production
Due to the federal deregulation of alcohol under Jimmy Carter’s presidency, there has been a boom of small producers across the country – usually called “craft producers.” Some of these craft producers have grown to be mega-brands in their own right, such as Left Hand Brewing and High West Distillery.
Craft producers are usually more transparent than the big producers. They are also more accessible – since they’re a local small business, you can call them up and ask a question about their production. They will know the answer to whether they use wheat in their craft whisky, for example. Calling up one of the mega-corps? Less likely to be successful.
Notes on Alcohol Types
I didn’t start drinking until I had conducted thorough research on how alcohol is made. Over the years, I’ve tallied up more insight into each category. This is hardly an all-encompassing explainer, but here are some notes on the major styles of liquor and some things to watch out for.
I’ve also done distillery tours in Scotland, brewery tours in the U.S. and Canada, and tours of craft producers in the U.S. This kind of information isn’t really something that is a Google search away (or, it would take you a lot of time to compile this – it’s taken me years!).
Visiting the Talisker Distillery on the Isle of Skye, Scotland
Wine
Wine is one of the most straightforward and well-regulated types of alcohol on the market. The primary allergen typically used in production are sulphites, which appear naturally in both red and white wines (although whites usually have far fewer).
Whether you’re buying a French Bordeaux, an Australian Shiraz, or drinking bottom-shelf wine from a box… wine is always made from grapes or other fruit, but if it’s made from other fruit, it has to be labeled as “fruit wine.”
Wine is harvested from grape plants and then dried out on large stands before adding yeast to ferment in order to produce alcohol. To make a sparkling wine like Champagne, they put the product in a bottle with more yeast to ferment further.
Wine is typically aged in glass, ceramic, concrete, stainless steel, or oak casks. They are allowed to add grape juice (or fruit juice) at some point in the production process and still call it wine, as well as Yellow No. 3 coloring and carmine (an additive).
There are a few odd wines I’ve seen in my time – an almond wine, for example (but they must label it as an almond wine since it’s not made from only grapes). But wine is typically a pretty straightforward alcohol for many people with allergens given the strict requirements on added flavors and production process.
A small vineyard in Tuscany that I visited in April 2022
Beer
Beer is more complicated.
The major brands like Bud Light have actually added a voluntary ingredients label (“Water, Barley, Rice, Hops.”) Traditional beer is made from malted barley. Barley, a grain crop, is harvested and then tricked into sprouting its sugary seeds using hot water. This is called malting. After the barley has been tricked, the brewer drains off the water filled with sugary barley, ferments it with yeast, and then makes it into beer. Most brewers also add hops, a bitter flower, for flavoring.
In 2015, the TTB modified its guidance and allowed beer makers to sell beer with many added ingredients as long as they were labeled on the package. This is about as close as you can get to an ingredients list. You can see a list here. And, you can see their guidance on how those additions might appear on a label here. Basically, there needs to be at least some description besides “beer” that notifies the consumer that there’s been fruit or spices added to the beer.
However! In recent decades, brewers have also used other grains to make beer – including wheat, rice, corn, oats, and rye grains. In this case, you might find beers that are called “wheat beers” or an “oatmeal stout” (which is a stout, a dark beer, brewed with oats). However, the beermaker is not required to list wheat or any alternative grain unless it comprises at least 25% of the grains used. That is particularly unfortunate if you have a particular allergy to a type of grain, instead of all grains.
This yields an unexpected trade-off in beer. On one hand – finding out that a mass-produced beer like Heineken is safe for you is very helpful, because they are going to make it the same exact way everywhere in the world and it’s a very simple recipe without any additives. They are using barley, water, and hops (and yeast). On the other, you can call up your local craft brewer and see what kinds of grains and additives they use and get clarity on what they put into the beer. But local craft producers might sneak in unusual ingredients.
I’ve seen plenty of craft beers brewed with peanut butter, hazelnuts, and other allergens. One particular ingredient for concern from craft brewers is lactose, which makes a particularly creamy kind of beer. It is not always labeled as a “lactose beer” or “beer brewed with lactose” so watch out for those! It is often mentioned in the description of the beer on the package, but sadly, they aren’t required to label it if they use lactose in production.
Liquor: Vodka
Vodka is a spirit distilled from, well, just about anything as long as it doesn’t have a distinctive taste or color and is bottled at 40% ABV or higher. Most vodkas are grain vodkas, meaning they are distilled from wheat or rye or barley. However, vodkas can be made from other materials like potatoes or sugarcane.
The good news is vodka must be labeled as flavored or have some other notice if they’ve added anything to it besides the base grain. So if you can have Grey Goose (made from wheat), it will always be the same Grey Goose if the bottle just says “vodka” and not “vodka flavored with X.”
Tito’s is a famous gluten-free vodka, made exclusively from corn. That’s a great example of a craft brand that’s become super popular in the last 20 years – originally started in 1995, Tito’s has become a big brand in the U.S. for vodka.
Craft vodkas have more variation than the megabrands in their spirit base. I can think of a local producer here who uses sugarcane, so it becomes slightly sweet, but most vodkas are a “neutral grain spirit” meaning they’re distilled from grain of some kind.
Liquor: Gin
Gin is tea made with vodka. You take an assortment of botanicals (such as juniper berries, eucalyptus leaves, flower petals, and so forth) and steep them in vodka to make a flavored vodka. After the steeping is complete, you re-distill the final product to produce a clear spirit that includes the flavors of your tea.
While juniper is the dominant flavor, a naughty little botanical can make an appearance in some gins – tree nuts. Both Beefeater Gin and Bombay Sapphire Gin contain almonds. There are many, many craft gins like Monkey47 that also contain almonds. Newer gins on the market such as Four Pillars’ gins contain macadamia or cashew nuts, and walnut is also known to make an appearance.
My saving grace has always been Tanqueray, a popular mass-market gin that doesn’t contain any nuts. I’ve also heard Aviation Gin, another popular mass-market brand, is safe.
Now, on the craft side, most producers take pride in the types of botanicals they put into the gin. Many times their website will actually list all of the botanicals used, so you might be able to actually identify all 22 botanicals used in The Botanist gin, a popular Scottish gin.
Generally though, to play it safe – this is one to avoid if you cannot do almonds. I’m grateful I can now eat these, but I’ve stumbled into many many gins that have almonds once I looked them up on their website. Let alone other niche craft gins that have other tree nuts!
A gin & tonic served up at a craft gin bar in Barcelona, Spain
Liquor: Tequila & Mezcal
Tequila is a heavily regulated product from Mexico, made entirely from 100% agave plant. Tequila uses agave from a specific region of Mexico and produces a sweet and vegetal spirit, while mezcal uses agave from a much broader region and is typically smoky (due to a different production process).
The regulations are pretty strict to call it tequila – of a bottle, only 1% can be additives like sugar syrup, glycerin, coloring, or oak extract. Any other flavorings or additives are a no-go. “Añejo” tequila is simply tequila aged in an oak barrel without any extra additives.
Mezcal has much looser rules and, given the explosion of craft mezcal, can be much dicier. I actually ran into a mezcal once at a bar that was made with peanuts (using a traditional mole sauce as a part of the production process). Cool idea, not great for me to be drinking. I discovered this because the bartend offered some for free, I politely declined, and then looked up the mezcal to learn more because “it tasted so good!” according to them. It’s uncommon, certainly, but a good reminder the craft producers are more likely to take risks in their production processes. The added benefit is the transparency they offer, but it’s always a risk to drink something you don’t know anything about.
From a regulatory perspective, tequila is much much more controlled. You could not get away with adding a mole sauce into the production of a tequila.
Liquor: Rum
Rum is broadly three types: clear/white/silver rum, aged rum, and spiced rum. All rum is distilled from sugar cane and molasses. Clear/white/silver rum are brand-new, unaged rums. Whereas aged rums, obviously, are aged (typically in oak casks).
Spiced rum is the troublesome category. Rum is actually pretty tricky to navigate with a nut allergy because there are many marketing designations that have no basis in regulation: dark rum, black rum, gold rum, etc. don’t actually mean anything.
Spiced rum is rum that uses spices, many times nuts. I believe Bacardi has five major rums and at least one of them contains nuts. The recipe for The Kraken (a popular spiced rum) is secret. Some rum brands are becoming more transparent, such as Captain Morgan, and disclosing what spices they use.
Craft rum is a saving grace here as many local distilleries who want to make whisky actually start out by making rum and gin first –– it helps pay the bills while the whisky ages. They will be able to disclose to you all the spices used if they create a spiced rum.
I generally avoid rum. Too many pitfalls. In fact, I think I’ve never had a mass-produced spiced rum. I have had one aged rum before. But if I’m out at a bar or a party, I’m not reaching for the rum. God only knows what is actually in the bottle.
Liquor: Whisky
By far the most regulated of the major liquors, whisky is dominantly American, Canadian, or Scotch. There is a big rabbit hole here, but essentially – all whisky is made first like beer, then distilled in copper stills and aged in oak casks, with varying requirements on time. If there are added flavors, it must be labeled. (Even Fireball is labeled “whisky with natural cinnamon flavor”)
Almost all major whiskies use a blend of grains, typically corn, rye, wheat, and barley. Bourbons must be made from mostly corn, rye whiskies from mostly rye, and single malt Scotch to be made from 100% barley. Blended scotches, such as Chivas Regal or Dewar’s, can be made from a blend of grains. However, different whiskies can use a different “mash bill” or combination of grains. The same producer might make one American whisky using corn/rye/oats and make another American whisky using corn/rye/wheat. And, they don’t have to tell you on the bottle.
Since whisky is always aged in oak casks, there are some variations. In America, the typical aging profile is “new American oak,” meaning it’s a brand new cask. Whereas in Scotland, they typically use “ex-bourbon casks” or “ex-sherry casks,” meaning the cask was previously used to age bourbon or sherry wine, and is now being used to impart flavors to the product. The casks types are heavily regulated – producers can’t simply throw it into anything.
There is a sub-genre of whisky that is aged in rum casks. I typically avoid these because I’m not 100% certain whether those casks were used for spiced rums (they never say, anyway). The only other whiskies I’ve ever been caught off-guard by are the flavored ones. Skrewball is a popular peanut butter-flavored whisky and Southern Comfort is flavored with tree nuts. There are all sorts of “flavored” whiskies and I drink absolutely none of them. Not even the Crown Royal apple-flavored one! The more standard whisky is better and safer as the production is heavily, heavily regulated.
A neat pour of whisky at canon, a bar in Seattle
Liqueurs
Typically a mad dash to see how fast you can have an allergic reaction. I’m only half-kidding. Liqueurs are generally a base spirit or liquor (wine and vodka are common bases) that have been infused with various additives, flavors, and other ingredients. Unlike gin, they are not re-distilled. They often retain the color of the infused ingredients.
Liqueurs are a black hole of information. Whether it’s cheap ol’ Malibu, Campari, Cointreau, Luxardo Maraschino, Strega, red vermouths, or blanc de blanc vermouths, there is very little transparency in the industry. Closely guarded “family recipes” mean there isn’t much information on what is used in the production of the liqueur. The recipe for one famous liqueur, Green Chartreuse, is only known by three people in the world (yes, really).
Liqueurs are also tricky due to their variations. Kahlua is a popular coffee liqueur. The original recipe does not contain nuts, but many seasonal variations they release contains nuts (like ‘The Mudslide,’ a riff with peanut butter). Many amaretto liqueurs use almonds, but not all. Disaronno, a popular amaretto, apparently uses cherry pits to achieve the same flavor without using any nuts (but who knows, really, and I haven’t had Disaronno before).
Most vermouths are wine that have been flavored with roots and herbs. I’ve never had a reaction to a vermouth, but I also don’t drink a lot of vermouths, so it’s possible some special vermouth has snuck in some nuts and nobody knows (yet).
Craft producers are absolutely your friend, as many are making “amaros” and “aperitifs” that achieve the flavors of these classic liqueurs like Campari or Aperol but have added transparency in the ingredients that they use.
Depending on your allergies, you may be left with a real “trial and error” system when it comes to liqueurs. Many craft producers have good alternatives to the mass-produced versions and added transparency on the ingredients they use.
Cocktails & Cocktail Bars
It’s a minefield, but the most common suspects for additional problems in cocktail ingredients (besides a liqueur) would be:
Orgeat, an almond syrup, that is used in popular drinks like the Mai Tai
Black Walnut Bitters and/or Coffee Bitters, a lightly alcoholic flavoring agent, that is used in some nicer bars for drinks
Ironically orgeat is a favorite ingredient in rum-based drinks, so you’ve got a real potential for a double whammy on a nut allergy if they’re also using a spiced rum that contains nuts.
A sensational craft cocktail at Stravinsky, a top 50 bar in the world in Barcelona, Spain
Craft cocktail bars can range in quality. But any bartend worth their salt will tell you that they cannot possibly know for sure whether the liquor and liqueurs used contain specific allergens. I haven’t had problems with many of the standard liqueurs like Campari or Aperol, but that doesn’t mean you won’t! Craft cocktail bars also use niche liqueurs that would be difficult to research on the internet.
On top of that, many standard bars do not practice hygienic cleaning. They rinse out cocktail shakers with water but most bars are moving so quickly, they usually mix equipment to make different drinks. The shaken martini for one client using a gin containing almonds will be measured in a jigger and poured into a shaker set; then, after a quick rinse of the shaker (and sometimes the jigger, but not always) they will make your drink. Is that safe preparation for someone with a severe food allergy? No.
More upscale cocktail bars are much more cautious and mindful about preparation, typically because they have multiple bartends on-hand. These environments have been more hospitable for me but it’s always important to tell them your food allergies!
Other Notes on Staying Safe
Ultimately the safest option is just not drinking. That’s probably the easiest! Here are some other notes.
Distillation reduces a lot of the protein, but not all, from added allergens.
Hardly medical advice, but a panel of EU researchers in 2007 studied 32 gins and found almond protein (when almonds were used) was not detected above 0.1 mg/L. As they say, “the Panel notes that proteins and peptides are not carried over into the distillate during a properly controlled distillation process.”
To me, this is small comfort for someone allergic to almonds. It may help avoid a very severe allergic reaction, but doesn’t guarantee someone will not react to protein inside. Also, this only really applies to gin? As noted previously, many of the products that actually “contain” nuts like spiced rums and liqueurs are not re-distilled after introducing the nuts. That means the presence of nut protein is way, way higher in those products! Gin is re-distilled, which helps reduce the amount of protein leftover.
Cocktail menus do not always list all the ingredients.
As someone who travels a lot and enjoys eating at new restaurants, do not take the menu’s word for it. Many cocktail bars add additional ingredients to the drink that are not listed on the menu. Make sure to always clarify your food allergies if you do order a craft cocktail, or stick with something safer.
Tasting notes or flavor profiles are not ingredients.
Often times you might run into a description of a whisky or a wine that mentions how “nutty” it tastes. This is almost always just a flavor descriptor. It is very, very rarely a description of what is actually used in the product. If it does actually contain nuts, it will be hinted at on the label (using “natural flavors” or a similar phrase).
Don’t drink if you don’t know it is safe.
Simply put, stick with what you know. I have never, ever accepted a mystery drink at a party. I do not order cocktails off menus with unknown ingredients. I stick with brands and types of alcohol that I know are safe. I always bring up my allergies when ordering drinks. If I’m at a less-hygienic environment like a dive bar, I’m not ordering cocktails period. I’m especially not going to take risks when alcohol is limiting my own cognitive ability to make good decisions or notice any symptoms to a reaction if they arise.
This is hardly a complete post on everything alcohol related, but I hope it was a helpful starting point for people who are navigating food allergies and alcohol! These are my own notes and experiences. You may have different experiences with alcohol. Please be safe!
I love the Fall – the changing of the tree colors, the temperature cooling down from summer heat, and when my children were little, the excitement of a new school year. Along with that love is the challenge of managing numerous conditions that flare in the Fall, if you’re like me and my family. Pollen allergies, asthma, Mast Cell Activation Syndrome (MCAS) and/or Eosinophilic Esophagitis (EoE) can heighten during the Fall season and be a beast to manage.
Near Lake City, Colorado
I’ve written previously about Mast Cells and the Fall Flare on this blog, and I’ve learned some new ways to manage the Fall Flare, so I wanted to write about this topic again.
The main new item that I can share, is that waiting until the Fall to manage symptoms that arise doesn’t work for me. By the time I’m feeling nasal congestion or the tightness in my stomach (from EoE), it’s difficult to take enough medication to calm down the symptoms without making myself feel sick. I need to pre-medicate, beginning in July, with small amounts of Zyrtec, Ketotifen (a mast cell stabilizer that also helps keep eosinophils at bay), and Nasalcrom. I slowly increase the dosage of these medications as I move into Fall to manage pollen allergies and MCAS symptoms.
For me, EoE isn’t a year round issue. It is at its worst in the Fall. I begin to use swallowed Flovent or Budesonide slurry every few days in July, slowly increasing the dose to twice a day as necessary through October when we have our first freeze or snowfall. Then, like magic, once the freeze comes my EoE symptoms disappear!
For my son, managing his asthma is a year round focus. Upper respiratory infections in the winter exacerbate his asthma, and pollen in the spring through the fall also can set him off. And of course, COVID is still roaming around, and he wants to ensure that his asthma is well managed should he get another round of it.
Year round, I see a Network Care Chiropractor to keep my nervous system calm. During the winter months, I go every 2-3 weeks. In the Fall, I see him every week! The Fall Flare really triggers my mast cells to activate, which in turn activates my nervous system to be on high alert. This makes sleeping difficult, and it also creates anxiety. It’s a bad combination and for years, I was almost unable to function through the Fall. Now I’ve learned to take the extra time to take care of myself and visit my doctor so that I can feel as well as possible during the high pollen season.
I have also increased my daily practice of Zhineng Qigong to 2+ hours a day. This practice has helped my body to heal so much since I started it 5 years ago. I have had several teachers through the years, however I do the practice solo most of the time in order to do the specific practices that help my body to feel good. Practicing year round has helped me to not only feel better in my body, but also to have a higher threshold when Fall comes around. What that means for me is that if I am stressed for several days on end, and the pollen counts are high, I’m less likely to have a mast cell meltdown where I feel like I can’t get out of bed. Lowering that threshold for triggers to create havoc has made my life much more livable this year! I ensure that I’m taking care of myself year round to be at my best health when the Fall Flare starts.
I hope all of you are taking care of yourself at this time of year and enjoying the beauty of Fall!
There’s a brand new book out called Allergic: Our Irritated Bodies in a Changing World by Theresa MacPhail. Theresa is a medical anthropologist – who knew there was such a thing ?! – and has done an admirable job covering topics from the medical discovery of allergies, diagnoses, where allergies might source from, treatments, research and more. I’ve just finished reading the book, and I’ve enjoyed reading it, and thought that my AllergicChild readers might benefit from what I found helpful in the book.
I’ve been in the Allergy World all my adult life, and have had years of experience with my own allergies and those of each of my children. Yet, I still learned more about the immune system and how it operates by reading this book. I also learned more about Dupixent and how it came into being. That was a fascinating part of the book to me. I’ve been wondering if it would be a good drug for me to try to combat my Eosinophilic Esophagitis (EoE) diagnosis. This book gave me more details than I’ve been able to find elsewhere. And my conclusion is that the price of the drug is still prohibitive for me!
Ms. MacPhail has interviewed literally dozens of the most esteemed allergists, scientists and researchers for the various topics she covers in this book. If you’ve been part of the Allergy World, you will likely recognize almost all of these individuals. It felt comforting to me that she went to the experts who shared their experience and specific research.
And beyond just the experts, she also interviews parents and advocates who have created groups and non-profits that help individuals in the Allergy World. I liked reading about these individuals, especially since I know them and have met them at food allergy conferences through the years. I respect them tremendously, and reading about them in the book only made me have even more appreciation for them and everything they have done for our community.
If you’re looking to learn more about food allergies, pollen allergies, your immune system and treatments that are on the horizon, I’d definitely suggest you read this book!
(PS – I’m not receiving any remuneration to provide you this review, nor do I know the author. But I would love to have more conversations with her if I ever did get to speak with her!)
This is a blog post that I’ve been intending to write for years. I wanted to share what we’ve experienced about helping our son, Morgan, learn how to manage visiting his allergist while he still lived at home. He could then make good choices about getting an allergist once he was out on his own, and Mom wasn’t around to give directions!
We’ve been blessed that Morgan was able to have the same allergist for 21 years, until he graduated from college. She watched him grow up and to learn to take responsibility for his health. However, it wasn’t until he was 19 years old, as a freshman in college, that he went to the allergist unaccompanied by Mom. Boy did it take work to get to that point!
Morgan visited with our allergist at least every 6 months throughout his life, beginning with his first appointment at 15 months old. He learned the routine of an office visit – fill out the paperwork listing all his medications, have a height and weight check, take a lung function test or two, and visit with the allergist to tell her how he’s feeling.
If Morgan had experienced any type of issue – a cold, virus or a pollen reaction – I wanted him to learn how to use his words to explain what happened. This was good practice for him to be able to explain to any adult what he was experiencing in his body and what he needed to feel better.
It took many years for Morgan to learn how to properly list all his medications that he took for pollen allergies and asthma, and to not forget any of them. He had to know the exact medication name, the milligrams, how often he took the medicine and whether he needed refills. I began having him complete this form when he was in grade school so that he could learn the details of his health needs. He would need to check with me about the answers, but he did all the writing.
Many times he would have school forms or camp forms that needed to be completed. He would complete parts of those forms, and I would fill in the rest until he was able to complete the forms by himself once he applied for accommodations in college.
It is vital that our children know all about their health condition(s), and are prepared to go to the doctor by themselves. Taking the initiative and the time when they are young to allow them to learn about the paperwork will help them later in life when they leave home.
It was at Morgan’s first allergist appointment that he had his first skin prick test. Holding down a wiggly, itchy toddler for 15 minutes was no easy feat!
From that test on, I kept an Excel spreadsheet where I input results from every skin prick, RAST and Immunocap blood test through the years. Every 3-4 years, we had repeat tests run. Because of the number of allergies that Morgan has, it has been helpful for him to refer back to this spreadsheet to see if he’s got an allergy to mold, or to some food that he wants to try. Then he can discuss the allergy test result with the doctor to see if a food challenge is warranted.
Once Morgan graduated from college, and moved to a suburb of Denver, Colorado, he needed to get a new allergist. He searched around and found a physician who knew our allergist. This doctor had been an allergist for over 30 years, and that made Morgan feel more comfortable. Morgan moved again two years later, and once again wanted to find an allergist near his home. This time, it wasn’t as easy to find a good fit. The first doctor he saw said that carrying just one autoinjector – Auvi-Q – was enough. That was enough for Morgan to decide this wasn’t the doctor for him. He knew he needed to always carry two Auvi-Q’s, and the fact that this doctor didn’t state that was concerning enough to leave the practice.
He decided to search for another doctor, and has now found a younger woman that he likes very much. She has redone all of his food allergy testing, and found that he is able to do an oral challenge for almonds. So far, he hasn’t found a desire for this. He continues to have food allergies to peanuts, tree nuts, sesame, fish and shellfish, and continues to see an allergist once a year and ALWAYS carries two Auvi-Qs with him everywhere.
I have full confidence that he knows how to manage his health, and he is fully capable of communicating with an allergist about all of his medical needs. And that was always the goal!
My son, Morgan, and his boyfriend, Quinn, returned from their vacation in London on Monday, March 16. If you haven’t read about that challenging return to the US, you can read about it here.
Both young men went home to self-quarantine after their return. During the trip, for a few days Quinn had been experiencing symptoms of fatigue, muscle aches, and a very low-grade fever, then he’d feel better. Since there was no way to get a COVID-19 test in England or Scotland during their trip, he just continued to enjoy the trip.
Morgan lives alone in an apartment in Westminster, a suburb of Denver, CO, while Quinn lives alone in Arvada, another suburb. Morgan felt sure that they had been exposed to the COVID-19 virus during their travels since they had been in planes, trains, automobiles and the Tube in London! They did their best to wash their hands and use the hand sanitizers available in many locations, however the nature of travel ends up with frequently being in crowds.
Morgan’s boss at the Longmont Economic Development Partnership had a baby while he was in London, and he returned to work early Tuesday morning handling not only his workload but hers also. His days were very long that first week back at work with numerous online meetings on the impact of the coronavirus on the local economy.
On Tuesday, March 24, he awoke with body aches, especially in his legs. At first he thought it could be from the yoga he did the previous day. Then, when he spoke with Quinn, he discovered that Quinn had been experiencing not only a stuffy nose but also a sensation of not being able to taste his food, which come to find out is apparently a strange symptom that many people with COVID-19 are experiencing. At that point, they were both convinced that they had the virus.
Day 2 of the virus, Wednesday, brought more of a tight chest for Morgan. He had been taking his inhaled steroid, Qvar, once per day but decided that he needed to check in with his primary care doctor to see what his next step should be and how to obtain COVID-19 testing. UC (University of Colorado) Health is a large network of hospitals and doctors in Colorado. They are providing telemedicine information and appointments for anyone with symptoms of the virus, in order to keep patients at home. Morgan called in to see where he could be tested for the virus and what he should do about the tight chest since he is diagnosed with mild asthma. He was told that there was no testing available in Denver unless he was hospitalized. As for the tight chest, the nurse with whom he spoke suggested that he increase his Qvar to twice a day. She also discussed what he should do if his breathing got more labored or he experienced wheezing, which was for him to call in for a telemedicine appointment with a doctor, who would likely prescribe Albuterol for his nebulizer. He was still working from home during all of this, trying to balance his need to rest with the workload.
As for Quinn, he didn’t have any new symptoms. He has no underlying health conditions, having outgrown asthma during puberty. He never has any issues with breathing troubles with a cold or illness. His strangest symptom was not being able to really taste his food. He was able to continue working from home all week without any fatigue or other symptoms.
Day 3 brought on a fever for Morgan who awoke with a general malaise, and a cough. When we spoke with him that evening, he sounded thoroughly exhausted. He had called back in to UC Health, in the middle of managing meetings for work, to request another telemedicine appointment for the next day, Friday. My husband and I hung up the phone quite concerned that the virus was really affecting him, and still clinging to the hope that he’d be able to stay in the “moderate” area of the illness. I posted on Facebook about both Morgan and Quinn having the illness and was pleasantly overwhelmed by the loving response of so many friends and family members concerned and sending prayers.
Day 4, March 27, was a lovely surprise to find Morgan feeling better. (My husband and I have a routine going where we talk with him every morning and evening!) He had decided to take the entire day off from work to rest, which in Mama Bear’s mind was a very good decision! He refrained from taking Tylenol the previous night, which he says upsets his stomach, and allowed his fever to spike through the night. He was up at 3 am taking a shower from sweating so much. But all that sweating helped him to feel much better on Friday morning. His cough was more productive sounding, and his energy was certainly better. I’m convinced all the positive energy coming from everyone also helped! His conversation with the doctor later in the day via telemedicine did not yield a prescription for Albuterol for the nebulizer. Instead, she suggested using a spacer and upping the Albuterol to 2 puffs, every 4 hours as a first step. It appears that doctors are trying to take small steps in fighting this illness to still have more available actions to tackle a worsening condition. We breathed a sigh of relief that his body was fighting off the virus, and by the evening he was feeling about the same, which we took as a good sign.
Day 5 is today, and his condition appears to have stabilized. He continues to say that he feels about the same. He is planning on resting all day today and tomorrow since it’s the weekend. Morgan hasn’t had to use the Albuterol inhaler at maximum dose because he has gotten relief from using it just a few times daily. The chest tightness has dissipated, and his cough didn’t even keep him up at night. He still has a slight fever that comes and goes. By the evening, however his cough was to the point where Morgan was having trouble talking without being interrupted with a coughing fit. We could hear him wheezing, which was really scary. He had been sitting in the bathroom of his apartment creating a steam bath for himself with hot water from the shower. He was also taking the Albuterol more frequently that day. We got off the phone that evening really concerned. In the middle of the night, I found myself awake wondering how EMTs would be able to get into Morgan’s apartment building since it is locked with no door person in attendance. I was in a very fearful place emotionally, and barely slept all night.
When we spoke to Morgan the next morning, Day 6, we decided to do so on FaceTime so we could see what he looked like. The telephone doesn’t provide as much information, we discovered, as being able to look into his eyes and to see how he was feeling. And thankfully he seemed to have turned a corner for the better. It was frightening how quickly the illness could turn from being stable to being really sick. And from what I read online, people who end up hospitalized for the illness, have on average been at Day 7. With that in mind, we continued to call him every morning and evening on FaceTime to check in over the next several days.
Morgan had several friends offer to get him food, however he only felt comfortable asking his sister, Michaela, to do so because she understands how to read a label for his food allergies (which are peanuts, tree nuts, sesame, fish and shellfish). She was able to get him groceries, dropped them off at the front door of the building while he gloved and masked up and picked them up.
Each day has brought him a little bit more energy, as he started back to work for a few hours building up to working all day by Thursday, April 2, Day 10. As of today, Day 11, he still has a cough, but the fatigue is finally gone. He’s also staying inside his apartment until he is completely free of all symptoms. One of the doctors he spoke to said that he should be free of symptoms for 72 hours before going out in public, and that he should be isolated for 14 days after the symptoms start. At this point, he still has several days to go to reach that milestone.
This weekend, we plan on having a virtual family dinner since we can’t get together in person! My husband’s birthday occurred while Morgan was in London, so we’d like to celebrate that. And we are certainly celebrating Morgan and Quinn both recovering from this illness!
As of now, I would say that Morgan experienced the “moderate” symptoms of the illness, while Quinn has enjoyed a “mild” illness. From what I’ve read, the mild or moderate illness will likely last 2-3 weeks, which doesn’t sound mild to me! And honestly, without either of them having access to a COVID-19 test, we are just assuming that they have that virus and not another influenza or cold-type virus. This is a very small sample size, but there does appear to be a difference in Morgan’s symptoms of chest tightness and coughing than what Quinn has experienced. Maybe that’s the difference in having asthma, since Morgan is prone to having asthma exacerbations with any type of upper respiratory illness.
I am so appreciative for all your wonderful energy in the form of thoughts and prayers for Morgan and Quinn! Stay home and stay healthy!!
The news of the Coronavirus (COVID-19) has begun to get my attention these past few days.
In general, I am not overly worried about the virus and its impact on my son with his well-managed asthma; however, he has been planning to go to London on vacation in less than two weeks. It’s a wonderful opportunity for him to share the city that he loves with his boyfriend, Quinn.
My son, Morgan, is now 24 years old, has mild asthma and multiple food allergies to peanuts, tree nuts, sesame, fish and shellfish. With the US Centers for Disease Control and Prevention official today stating that “It’s not so much a question of if this (coronavirus) will happen any more, but rather more a question of when this will happen and how many people in this country will become infected and how many of those will develop severe or more complicated disease,” I realized that it’s time to have a conversation with Morgan.
Morgan and Quinn have plans to go to Britain for 10 days in March, and everything is planned, paid for and reserved. Waiting for the day to leave was the only thing left do do until this Coronavirus outbreak occurred. Now there are a few more things to prepare for just in case there is an outbreak of the virus in Britain while he is in the country.
Since Morgan is a young man now, Mama Bear here can no longer dictate his life…and truthfully, I never really had that power even when he was young! I thought it would be beneficial for the two of us to have a conversation about the virus, and so I asked him “What have you thought about the Coronavirus and your plans for going to London?”
I must say that I was impressed that he said that he and Quinn have been having conversations about how to stay healthy with hand washing, bringing wipes, and probably wearing a mask especially in the Tube in London where they will be near so many people. Morgan said, “I am nervous to travel. I don’t want to be stupid.” The two are closely monitoring any travel bans, and keeping up with the WHO recommendations and with the BBC for news on the virus in Britain. He recognizes that just like with influenza, his asthma is a health condition that can be exacerbated with the virus and is a cause for concern.
But, it’s now his decision as to whether or not he wants to reschedule his vacation. There are no travel warnings as of this writing for Americans going to Britain, and both of our countries have individuals who have been diagnosed with the virus. Thankfully both countries also have very good medical systems, which from what I have read, has helped those patients who do have a more severe form of the virus requiring hospitalization. And good medical care also keeps the virus from spreading to other individuals.
I have two N95 respirator masks to give to him for their trip. Two days ago, I tried to purchase more of these types of masks, which are rated the best for keeping out small particles including virus germs, and there aren’t any available in my local stores. Every Home Depot, Ace Hardware and Lowe’s is sold out already! I managed to find the masks online only through an individual seller on Ebay and purchased several more for the entire family at a reasonable price. Sadly, many sellers on Amazon.com have increased their prices to double or triple the regular price of a mask, if you can find any in stock.
Morgan has been taking Qvar daily, and has a prescription also to Albuterol. I suggested that he contact his allergist to find out if the doctor has any other suggestions for him especially if he ends up getting the virus here or abroad.
Another item we talked about was what he should do if he were to be quarantined in Britain. These quarantines have begun to hit various cities in numerous countries when an individual gets sick with the virus. People have been quarantined in China, but also in various other countries, and have lasted anywhere from 14 days to a month. With food allergies, not having access to safe foods is a serious issue, and one that requires some forethought as to how that situation would be negotiated in a hotel, for example. Morgan is putting together an action plan on how to manage such a plight. He and Quinn will be staying in an Airbnb for part of their stay and in a hotel for the remainder. It would be a real mess if they spent their vacation locked in a hotel room!
Morgan is going to check into the National Health Service (NHS) to see how an American can access these services should he need to. From his recollection with studying abroad at the University of Lancaster in Britain three years ago, it was fairly easy and inexpensive, unlike the US healthcare system!
There are a few pieces of good news in all of this. First, thankfully the mortality rate is fairly low for this virus versus previous coronaviruses like SARS or MERS. No one enjoys getting sick, but most people are surviving this virus. And secondly, Morgan has another 10 days to gather more information and to watch the spread of the virus to determine whether he will be heading to London or rescheduling his trip!
Morgan was 10 years old the end of January 2006 when this article was written originally for our February newsletter. He was then anaphylactic to peanuts, tree nuts, sesame and shellfish. He is severely allergic to dogs, cats and other furry animals. He gets eczema from food dyes, has mild asthma and is allergic to grasses, weeds and trees.
Where are your EpiPens® kept at school?
Just in case if I have an allergic reaction at school, I can use them. They are not by my side in the school. Two are in the office – one to stay there and one to go out to the playground with the monitor. I don’t think that is the greatest place to put them though because they are locked away. I also have one in each of my classrooms. (Mom’s note: in 2006, it was not legal for Morgan to self-carry his EpiPens, therefore other arrangements had to be made. It wasn’t until 2007 that he began to self-carry).
Do you trust that your teacher would know what to do if you were to have an allergic reaction?
Yes I do.
Do you trust the office staff to know what to do?
Not really. We had a boy a little older than me that had an allergic reaction and they did not use his epinephrine. They thought he had the flu. He did not die thankfully.
When you get older, do you plan on teaching your friends how to administer an EpiPen®?
YES I do! So they know what is happening when I’m in shock and what to do. Usually one of my friends is close by at all times.
What did you teach your Cub Scout Den about emergencies and food allergies?
I taught them how to use the EpiPen® and when to use it. I taught them the process which is put the EpiPen® in my thigh, call 911.
With the recent death of a girl dying after kissing a boy who had eaten peanut butter, what different behavior will you practice when you get older?
I’m never going to date a girl who eats peanut butter all the time. It is just too dangerous.
Will it be difficult to tell a girl what she can eat?
No. Not necessarily. It won’t be that hard just because it is a situation between life and death. I don’t want to risk my life.
Recently, my son, Morgan, and I spoke at a FARE Community Engagement Council event in Denver on “Preparing for and Going to College with Food Allergies.” It was a wonderful event with dozens of attendees – both parents and teens – managing food allergies.
We shared first about what parents can do to prepare their child for college during grades K-12. You can read that blog post here.
Then, we spoke about how to go to college with food allergies, and the necessary steps to find out the information about food allergy awareness at a school.
I am frequently asked how to begin searching for a safe college when you/your child has food allergies and/or asthma. What questions do you ask when you visit a college? When should you ask these questions?
It was very important for me to remember that my son was the one going to college, so he and I had several conversations prior to visiting any college about what he wanted to learn during a college visit. I asked him to develop a list of questions that he had for college officials about living arrangements, eating in the cafeteria and academic interests. We then compared our lists and came up with the following questions pertaining to the food allergies and asthma. Your list may also include specific academic interests.
Here’s a list of questions on food allergies and asthma that are useful when visiting a college:
Are ingredients listed on all foods served in the cafeteria? If not, is there an app or a website that will have the ingredients?
Is there a chef on site to take special orders?
Are the cafeteria workers trained on food cross-contact?
How many of your child’s allergens are regularly served?
Can my child and I speak with a dining manager about my child’s needs?
How old are the dorm buildings and cafeteria facilities?
Has there been any water damage or flooding in the past?
Are the dorms air-conditioned? (If not, what documentation will be necessary to submit for a medical necessity to live in air-conditioning?)
Are pets (such as dogs and cats or other emotional support animals) allowed in the dorms?
Can the resident adviser be trained on the administration of an epinephrine auto-injector?
Is stock epinephrine carried by security personnel on campus?
Can roommates be selected to ensure no food allergens are in the dorm room?
How is a 911 call handled on campus?
Is food allowed in classrooms and lecture halls?
Is smoking allowed on campus?
What paperwork is necessary to complete for the Disability Services Office to provide accommodations?
Yes, this is a long list of questions, yet you may have more depending upon your child’s allergies and needs.
When do you ask these questions?
I’d suggest first starting with the college website. If you go to the Dining Services page on the college’s website and find NOTHING about food allergies, that is your first clue that you may have an uphill battle. Schools that are aware of food allergies put that information on their website along with who to contact to ask questions.
The Housing page on a college website will generally not have any information about food allergies, but will likely have a contact person for questions.
We found that Disability Services website pages are usually geared more toward those with learning disabilities; however a few schools are starting to incorporate information about food allergies and what paperwork will be necessary. We waited until our son was accepted into his school of choice to begin specific conversations with Disability Services about our son’s situation. While a school should not deny admittance because of a disability, there’s no reason to give too much information prior to acceptance.
We found it best to have specific appointments set up with the Housing Office and with Chefs in the Dining Hall when we visited a campus to learn more about how they managed students with food allergies. Prior to him being accepted, we only asked general questions about what accommodations could be expected for a student with food allergies and/or asthma.
As for the Disability Services Office, we visited with a representative after my son was accepted to the school. We asked very specific questions about paperwork necessary for our son to receive accommodations. We found out that many schools will require that your child have recent testing confirming food allergies and asthma if specific accommodations are being requested. In other words, a skin prick test from 10 years ago was not going to suffice. A letter from our allergist delineated the specifics of what Morgan was going to need to safely attend college. The Disability Services office paperwork is best completed in the summer prior to the school year starting so that everything will be established once school starts. And remember that everything is completed and driven by your child once they are 18 years old. Schools expect your child to advocate for themselves.
Most colleges in today’s environment have managed students with food allergies. That can be a good thing if your child expects to eat in the cafeteria. It can be a negative thing if the college expects your child to have allergies similar to other students they’ve encountered, and you want a different accommodation.
There are several other lists of colleges and their accommodations for students with celiac and/or food allergies that might be helpful. Of course, it’s always preferable to use these lists as a guide and to visit the college yourself to ask questions specific to your child’s needs.
I have recently begun speaking with local Colorado Springs, Colorado Allergists and their staff regarding the large number of teens and young adults who have died from anaphylaxis.
I wrote an article for Allergic Living, Teens Speak Up About Averting Food Allergy Tragedies, which showed me that too many teens aren’t taking the precautions necessary to keep themselves safe; however, the teens did state that they listen to their parents and their doctors about food allergy information.
In Dr. Ruchi Gupta’s newest survey of parents, which she titled, Parents in dark about using epinephrine for kids’ food allergies, she found that “Less than 70 percent of parents recalled their allergists explaining when to use epinephrine and less than 40 percent said the same of their pediatricians.” Therefore, I question whether teens and young adults are getting good information from their parents.
Therefore, I felt it was time to bring this information to the attention of allergists in my area.
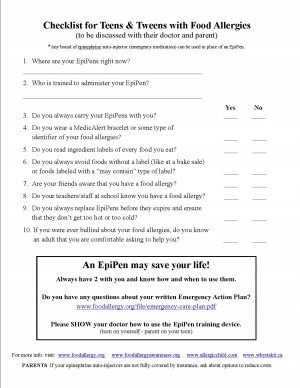
Here is the checklist I’ve suggested for allergists to discuss with parents, kids, teens and young adults who have food allergies, EVERY TIME they see the patient. Similar to an asthma checklist, which my son completes each time he sees our allergist, this checklist would be given to the patient to complete and review the gaps in behavior that could potentially create a life threatening situation.
A PDF version of this checklist is available here.
From what I’ve found, allergists in my area are not currently reviewing these items with their food allergy patients. In an educated patient, the checklist could be reviewed quickly and rewarded with a high-five or fist bump! In patients who need more awareness, the allergist can remind the parent and child/teen or young adult which behaviors are risky and where to make changes.
If a food allergy patient isn’t seen but once a year to get an EpiPen prescription refilled, then it is especially important for the physician to review these questions to ensure safety. I’m convinced this would begin to educate the patients and parents who so desperately need to hear from their doctors how to practice vigilance.
Please FEEL FREE to share this with your allergist and/or pediatrician and help to save a life!
If you haven’t heard of Traditional Chinese Medicine, you’re in for a treat! And if you have, you know that Henry is the author of “Food Allergies: Traditional Chinese Medicine, Western Science, and the Search for a Cure”. Henry graciously offered to answer a few questions about this treatment option for eczema, food allergies, mast cells and even Eosinophilic Esophagitis!
First of all, Nicole, thanks for giving me this opportunity to communicate with your readers. I hope they will find it informative.
The six most obnoxious words in the English language are “as I say in my book” so at the expense of stealing my own thunder…. I met Dr. Li when I went up to her office at Mount Sinai at the suggestion of my cousin and co-author of an earlier book, Dr. Paul Ehrlich, a prominent pediatric allergist. We also had a new website, AsthmaAllergiesChildren.com, and he told me, “I have been practicing for over 30 years and this is the first thing that sounds new and hopeful to me.” So I met Dr. Li. When she showed me photographs of the dramatic changes her therapy had made on really bad atopic dermatitis, I knew something was up. I mean, these were bleeding, sores on the feet of a ten-year-old girl. Within a few months, the skin was clear and she was painting her nails. I have a daughter. That means something to me.
How is Oral Immunotherapy (OIT) different from TCM?
OIT, like all immunotherapy, works by essentially over-stimulating the part of the immune system that produces allergic antibodies—allergen-specific IgE—by feeding progressively larger doses of the allergen until it can’t keep up with demand, allowing the part that produces tolerogenic antibodies—IgG—to gain the upper hand. Instead of allergen-specific IgE occupying the receptors on mast cells and basophils, IgG starts to occupy them instead. Allergens that once triggered reactions by connecting with IgE on those cells are rendered harmless.
Traditional Chinese medicine as practiced by Dr. Li works on modulating the immune system. There are two kinds of helper cells involved, Th1, which helps fight infections, and Th2, which is associated with allergies. In a normal immune system, IgE is a tiny fraction of IgG. But for various reasons, Th2 and IgE gain a disproportionate share of immune response. Dr. Li’s therapies restore Th1 and Th2 to their natural equilibrium. Oh, and one thing I have to stress is that Dr. Li also treats digestion so that the gut has a better chance of breaking down allergenic proteins before they can be absorbed into the blood stream and find their way to different parts of the body.
Let me add that immunotherapy and TCM are not competitive or mutually exclusive. TCM patients are also receiving OIT, just as they are receiving shots and sub-lingual immunotherapy. There’s no single therapy that will help every patient in the long run.
How long has Traditional Chinese Medicine (TCM) been used by Dr. Li to treat patients for food allergies?
Her private, independent clinic got started to treat recalcitrant eczema while she did more conventional research in her “day job”. However, in the mid-1990s, food allergy mothers she met at a fundraiser for the Jaffe Food Allergy Institute, where she was doing research, upon hearing of her success with eczema, told her their kids’ stories and she was so moved she set out trying to find ways to help, backed by Dr. Hugh Sampson, her boss. It was a very bold move. Dr. Li was trained in both western medicine and TCM. She looked to the classical TCM formulary for answers, and started to find them, starting with a treatment for intestinal parasites. It is important for your readers to understand that while Dr. Li is following all the NIH protocols for her investigational drugs, she is also allowed to use versions of these medicines as supplements in her clinic.
Is she working on having fewer pills to take/teas to drink as part of her protocol?
Yes, Nicole. One of the problems with these treatments is that because they are derived from plants, therapeutic doses require lots and lots for prolonged periods. Compliance is a challenge for all of us, whether we have diabetes, asthma, or even just take a low-dose aspirin (as I’m supposed to do—don’t tell my doctor). Dr. Li works with her own lab and scientists in China to refine the medicines and reduce the burden on patients. Her food allergy herbal formula-2 had a dosage of 10 pills, three times a day for a phase-2 trial. Lots of subjects had trouble. The next trial will use B-FAHF-2–refined with butanol, a form of alcohol—that will take the dose down to six or eight pills a day total. Much easier.
Have there been any patients on TCM long enough to say that their immune system has been remodeled, and they are no longer allergic to foods?
Yes there have, although most of her patients have complex co-morbidities—and it’s a work in progress for many of them. I suggest your readers also check out an article published last year in a Canadian journal about three cases of frequent severe food anaphylaxis to see how dramatic the changes can be.
In a video at last year’s Food Allergy Bloggers Conference, you and Dr. Li were interviewed for a podcast. Dr. Li mentioned using TCM for patients with Mast Cell Activation Disorder (MCAD). Has she had any success with patients with this condition?
In the new book that Dr. Li and I have co-written, there is case of this, also called mast cell activation syndrome. Just so you know, MCAD or MCAS for mast cell activation syndrome is disease in which mast cell degranulation is triggered by all kinds of things, from foods, to exercise, to heat…really lots of things. It didn’t even have a name till 2010 or a practice parameter till 2011. It can be IgE mediated or not. We have one whole chapter in our book devoted to one case of a girl of 14 who suffered for 5 years without a diagnosis even, and almost died. Dr. Anne Maitland, a colleague of Dr. Li’s, is gaining a reputation as an MCAS specialist, and the two of them are doing great work. The case we write about it the book will tug your heart strings.
What about children with Eosinophilic Esophagitis (EoE) – are they able to tolerate the herbs? Have any children been ‘cured’ of their EoE?
The short answers are “yes” and “yes”. In my first book I have a case of a boy who was successfully treated, and according to his mother now has the enviable position of being able to eat pizza every day with his friends. Before he couldn’t tolerate dairy.
Let me add a key point here—all Dr. Li’s treatments are highly individualized. You don’t go in and get the food allergy pill, or the asthma pill, or the EoE pill. You get a combination of things that help with the multiple organ systems that are involved. The herbs overlap, and so do their effects.
And one more critical point: Dr. Li is a full-time scientist and a part-time healer. The scope and ambition of her research is breathtaking. Her chemists and biologists love working for her. A month doesn’t go by when I don’t hear about something new emanating from her lab or suggested by researchers elsewhere who have been following her work.
Tell us about the new book you are writing – when should we expect it? What’s the topic?
Think The Godfather and The Godfather Part 2, where the sequel is as good as the original. This book updates the food allergy research from the last book but also goes into greater detail on ASHMI—anti-asthma herbal medical intervention, which I only wrote about briefly the last time. But it’s huge for people with this condition. It also goes into the atopic dermatitis treatment at length, Crohn’s Disease, MCAS, and some other things. I wrote the first one the way I did because I was learning the science on the fly, but this story is much bigger than any single allergic disease. Dr. Li is getting an award next year from the Future of Health Technology Institute, which is normally very high-tech and where the people obviously see this as very important for the way we understand and treat disease. The new book will be out some time in 2016. After writing two books in three years, don’t expect a third one any time soon, although I know if there is it will be better than Godfather Part 3.
Henry Ehrlich is the editor of asthmaallergieschildren.com and co-author of Asthma Allergies Children: a parent’s guide and half a dozen other books. He was a long-time professional speechwriter, with three grown children and one granddaughter.
There is an abundance of research trying to find a cure for food allergies. Because of the stomach issues in our family, mast cell disorders and EoE, we have chosen to seek out different healing arenas than eating what we’re allergic to.
About a year ago I began seeing a chiropractor that practices Network Spinal Analysis (NSA). For those of you who have read my blog for a while, you know that our family is very open to new modalities of healing AND we still see medical doctors too!
We have spent a lot of money seeing NAET specialists (see my write up on that here toward the bottom of the page), acupuncturists, chiropractors, Sacral Occipital Therapists, massage therapists…the list goes on and on. Many of these practitioners have provided temporary relief, at best. And the abundance of them have served only to lighten our wallet! I know that my son needs to have medication to manage his ocular allergies, his asthma and his nasal allergies; however, I’m always on the lookout for something that can assist his body to truly heal from these maladies.
My daughter and I have a mast cell disorder, and I was having severe lower back pain that wasn’t being helped by traditional chiropractic care. I decided to try something new and be the guinea pig in the family. It turns out that the mast cell disorder and the back pain were related, according to my new NSA chiropractic doctor. The more allergic reactions I was having, the more mast cell proliferation occurred. And the more mast cells, the more my back hurt. It was as if my spine was shutting down my entire nervous system in an attempt to protect me from myself!
Network Spinal Analysis works to utilize the energy in the spine to realign itself without the standard “cracking” of a chiropractic adjustment. The practitioner helps to point out where the energy is blocked, and gets the central nervous system to pay attention in an entirely new way. New neural pathways are opened up, and more energy is brought in to the spine, so that healing can occur. Within a few months, my back pain ceased, and almost a year later, my mast cells are beginning to behave better too.
Last summer, my son, Morgan, began seeing this NSA chiropractic doctor and almost immediately was able to go off of his Pulmicort steroid. I wasn’t sure that was a good idea until we went in to see the allergist and all of his breathing tests were normal!! He has had to use a rescue inhaler only once since then for a few days during a respiratory infection. He’s had no chest tightness, and feels great.
I really believe there is something to raising the energy in the body to create healing. Let’s face it, all the antihistamines and steroids are doing is helping with the symptoms. I really want my body, and my son’s body, to begin healing. Since Morgan and I had such good results with this new modality, my husband and daughter have also begun receiving entrainments (what the doctor calls the session). They too have had remarkable results with less body aches, better digestion and overall energy becoming higher.
There’s another line of thinking about accessing a higher energy through meditation to create healing. Dr. Joe Dispenza has written a book, “You Are the Placebo” that asks, “Is it possible to heal by thought alone—without drugs or surgery? The truth is that it happens more often than you might expect.” His book details scientific research where people have healed themselves, and where others have made themselves sick, simply by their thoughts and beliefs. I know that my mind is certainly powerful enough to create anxiety symptoms in my body. It’s powerful enough to create a stomach ache out of fear or worry. It’s also powerful enough to boost up my energy and overall capabilities to handle a crisis of one of my children, regardless of how I’m feeling physically in the moment.
I have begun to sit in meditation daily for the last 4 weeks, based upon the guided meditation provided in the book. I’ve already seen and felt a difference. I’ve been able to decrease the amount of medication that I take for my mast cell disorder! It’s mind blowing stuff, when you really think about it. Are our minds really powerful enough to heal our bodies? I am becoming a believer!
When our son, Morgan, was 3 weeks old he was diagnosed with RSV – Respiratory Synctial Virus. It was a frightening illness that landed him in the hospital with oxygen necessary around the clock and nebulizer treatments every 4 hours. The illness lasted for three VERY LONG weeks. Thankfully, Morgan fought through the illness and still gained weight like a champ!
Nine months after this occurrence, Morgan touched a peanut butter sandwich, reacted with hives, and we were baptized into the food allergy world.
At 18 months old, Morgan got a horrible cold that got considerably worse during a blizzard that we had. (We are in Colorado, so blizzards aren’t uncommon occurrences). My mother was unable to get home from work, and stayed at our house that night. All through the night, I got up to check on Morgan and his breathing. I knew by the early morning hours that he needed to get to at least get to our doctor’s office. My Mother thought I was crazy. She was accustomed to letting kids just battle through illnesses. I had an instinct that something was clearly not right, and listening to my Mother could have had disastrous consequences. I got into the doctor’s office and we were able to thwart off the need for oxygen thankfully. Morgan was given a large prescription for nebulized albuterol to have on hand for any future similar occurrences.
Morgan continued to have bronchial spasms every time he got a cold, which was eventually diagnosed as mild asthma at about age 3. The impact of RSV, food allergies and asthma was much more problematic for me – aka Dr. Mom. I was forever scared that every sniffle was another major illness requiring an emergency room run. It was difficult to know when to get him immediately into the doctor and when to allow a virus to run its course.
Morgan also had strange reactions to illnesses. He would break out in hives during a virus, for example. Or he would be the only family member who didn’t get sick when everyone else was sharing the germs. I don’t understand everything with the immune system, yet I have learned that children with food allergies just don’t respond the same to illness that other children do. Either Morgan’s system goes way overboard, or he doesn’t react at all.
In the elementary school years, Morgan would want to stay home upon the first touch of an illness. Maybe he felt better at home – almost like he didn’t trust what his body was going to do and he’d rather be at home when something happens! Children at this age are sick so frequently, but I really felt better being able to watch over him.
As he aged into high school, he was more able to handle illness and go to school when he had a cold. And I’ve learned how to let go a little more and realize that not everything necessitates Dr. Mom’s hovering presence!
This past weekend was another one of those scary illness times. Morgan had been at a Speech/Debate tournament all afternoon Friday and into the evening until 11:30pm. He was up very early and back at the tournament by 7:30am Saturday morning. I didn’t see him Friday night or Saturday morning, but I had a sense that he was going to be getting sick. Call it Mom’s intuition. He’s been cramming a lot of activities into his schedule during his last semester of high school, and sleep is frequently missed.
He had 6 rounds in the tournament and he won every round, which no one else was able to do. This means that he will be going to the National Speech/Debate tournament in June. He was thrilled with his accomplishment and must have let out a large sigh of relief.
Then he called me and said that he was so sick that he didn’t think he could drive home. He had chills so bad that his teeth were chattering. I had no idea what illness he could have that was causing such dramatic symptoms so quickly! I drove over to the tournament, which was thankfully in our same city. My husband talked to Morgan about coming home and not staying for the awards’ ceremony. That was a big disappointment for him since he worked so hard, but we needed to get an assessment of what was going on and we wanted to keep the other participants healthy.
We took him to an Urgent Care facility. The doctor determined that it was possibly Strep Throat. Since Morgan had two college scholarship interviews occurring all day Monday (about 36 hours later!), we asked the doctor to put him on an antibiotic immediately even though the Strep Test came back negative. The doctor understood the situation, and graciously agreed!
Morgan slept for 16 hours, got up the next day feeling a little sluggish but knew that he was on the mend. The Strep Test never did show as positive, but the antibiotics worked and he was able to make it to the Scholarship Interviews early Monday morning.
I’m sure we will one day be able to laugh about this past weekend, but it was harrowing to watch him so sick and pale. We can add another crazy immune response to Morgan’s list of odd things – he never tests positive for a strep test even though he has the illness!
Dr. Hemant Sharma is the Associate Chief of the Division of Allergy and Immunology at Children’s National Medical Center in Washington, D.C. He is also the Director of the Food Allergy Program and site director for the National Institutes of Health Allergy and Immunology fellowship program. Dr. Sharma obtained his medical degree from Columbia University, and completed his pediatric residency and chief residency at Duke University. He trained in allergy and immunology at Johns Hopkins, where he also completed a degree in clinical epidemiology. He is a regular contributor to a food allergy column in Allergic Living magazine and recently co-edited the “Food Allergy in Children” series for Pediatric Clinics of North America.
Dr. Sharma, thank you for helping us to learn more about asthma and food allergies. Dr. Ruchi Gupta’s recent research found that nearly 8% of US children under 18 have food allergies. Do you know of recent research that has determined how many children with food allergies also have asthma? In your practice, how many children have both?
Food allergies and asthma often do occur together. Prior studies suggest that more than a third of children with food allergies also have asthma, and up to 8% of asthmatic children have a food allergy. It is not uncommon for us to see something called the “atopic (or allergic) march” in children, where they start out in infancy with food allergy and then go on to develop asthma and hay fever later in childhood.
My son had Respiratory Syncytial Virus (RSV) at 3 weeks old. We heard that this would make him more likely to have asthma. Is this true? Is there any relationship between RSV and food allergies?
RSV infection in infancy has been shown to be associated with a higher chance of developing asthma later in childhood. Interestingly, wheezing with rhinovirus (the common cold virus) in early childhood is actually a much stronger risk factor for later asthma than RSV. It’s not entirely clear if these viruses cause asthma or are simply predictors of childhood asthma. There is not any evidence for a connection between RSV and food allergy.
Is asthma the same as “reactive airways”? Is it medicated the same?
The term “reactive airways” is often used by health care providers to describe wheezing in early childhood, when it may not yet be certain whether that wheezing will resolve over time or develop into chronic asthma. One of the hallmarks of asthma is reactivity or “hyper responsiveness” to triggers, which can lead to tightening around the airways during a flare-up. Both “reactive airways” and asthma may be treated with the same medications, for example bronchodilators like albuterol, which help relieve this tightening around the airways.
Is there a different protocol for your patients who have just food allergies versus those who have both food allergies and asthma? How about children who have the atopic trifecta: food allergies, asthma and eczema?
The management of food allergies is similar whether a child has food allergies alone, or accompanying asthma and/or eczema. Food allergen triggers should be avoided, and in some cases, this may help to improve eczema control as well. In addition, emergency medications to treat food-allergic reactions should be available at all times, including epinephrine, antihistamine, and, if a child has asthma, albuterol. For children who have both food allergy and asthma, asthma symptoms might certainly be part of a food-allergic reaction, but they are usually not the only symptom observed.
My son has severe peanut & tree nut allergy – among several other foods – and mild asthma. I’ve read that two of the risk factors for fatal anaphylaxis are peanut or tree nut allergy and asthma. (The third being a delay in the administration of epinephrine). Why are peanut/nut allergy and asthma implicated with this higher risk of a fatality? What should my son be doing to mitigate this risk?
Certain foods, like peanuts and tree nuts, have been shown to be associated with a higher risk of fatal reactions. The reasons are not entirely understood, but likely are related to unique biochemical properties of these allergens. It is also important to note that fatal reactions have occurred to many foods other than nuts. Asthma is another risk factor for fatal food allergy reactions. This might be explained by delayed use of epinephrine since people with asthma might often reach first for their inhaler when they are experiencing breathing difficulty, and overlook other signs of anaphylaxis. For patients with both food allergy and asthma who develop abrupt respiratory symptoms, it’s advised they assess whether other symptoms of anaphylaxis are being experienced, and if so treat immediately with epinephrine.
For years we thought that my son had outgrown his asthma. When we went to National Jewish Hospital a year ago, he had a Nitric Oxide test that our local allergist wasn’t able to administer in her office. We then found out he had likely had mild asthma all along and had gotten accustomed to a tight feeling in his chest. Our allergist’s testing methods weren’t refined enough to pick up the problem, and my son didn’t know he was having difficulties. Should we parents be looking for certain signs of asthma if our children have other allergy issues?
The most commonly used test to evaluate lung function in asthma is spirometry. This form of lung function testing measures obstruction to air flow, usually before and after receiving a bronchodilator medicine, like albuterol. Nitric oxide testing, instead of measuring obstruction, detects airway inflammation, which might be present in uncontrolled asthma. While this test may provide useful information in some cases, it cannot by itself diagnose asthma, and is not a test that needs to be done for every child with asthma. In fact, studies have not shown that using nitric oxide testing helps to improve asthma control, beyond relying on a thorough assessment of symptom frequency, need for albuterol and spirometry results.
There is more research recently to find a cure for food allergies. I’ve read that asthma kills 9 persons a day sadly, in the USA alone. What research is there to find a cure for asthma? Do you see any great new asthma medications on the horizon?
Research is also under way to identify new treatments for asthma. Omalizumab (Xolair) is an example of a new asthma medication that has helped patients with severe allergic asthma, who failed to respond to other asthma treatments. It functions by blocking the binding of the IgE antibody. This medication is also being studied for potential use in food allergy.